DPP-IV inhibitors improve blood sugar control by preventing the breakdown of incretin hormones, while GLP-1 agonists mimic these hormones to enhance insulin secretion and suppress appetite more effectively. Your choice between these treatments depends on factors like efficacy, weight effects, and side effect profiles, with GLP-1 agonists often providing greater weight loss benefits.
Table of Comparison
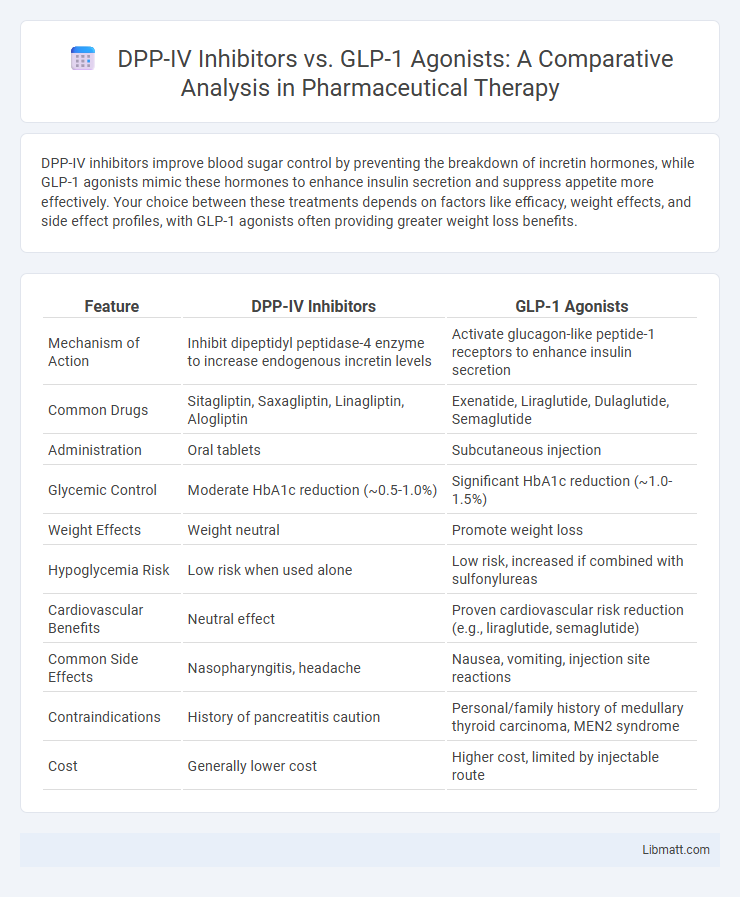
| Feature | DPP-IV Inhibitors | GLP-1 Agonists |
|---|---|---|
| Mechanism of Action | Inhibit dipeptidyl peptidase-4 enzyme to increase endogenous incretin levels | Activate glucagon-like peptide-1 receptors to enhance insulin secretion |
| Common Drugs | Sitagliptin, Saxagliptin, Linagliptin, Alogliptin | Exenatide, Liraglutide, Dulaglutide, Semaglutide |
| Administration | Oral tablets | Subcutaneous injection |
| Glycemic Control | Moderate HbA1c reduction (~0.5-1.0%) | Significant HbA1c reduction (~1.0-1.5%) |
| Weight Effects | Weight neutral | Promote weight loss |
| Hypoglycemia Risk | Low risk when used alone | Low risk, increased if combined with sulfonylureas |
| Cardiovascular Benefits | Neutral effect | Proven cardiovascular risk reduction (e.g., liraglutide, semaglutide) |
| Common Side Effects | Nasopharyngitis, headache | Nausea, vomiting, injection site reactions |
| Contraindications | History of pancreatitis caution | Personal/family history of medullary thyroid carcinoma, MEN2 syndrome |
| Cost | Generally lower cost | Higher cost, limited by injectable route |
Introduction to DPP-IV Inhibitors and GLP-1 Agonists
DPP-IV inhibitors work by blocking the enzyme dipeptidyl peptidase-4, which breaks down incretin hormones, thereby enhancing insulin secretion and lowering blood glucose levels in type 2 diabetes patients. GLP-1 agonists mimic the glucagon-like peptide-1 hormone, stimulating insulin release, suppressing glucagon secretion, and promoting satiety, leading to improved glycemic control and weight loss. Both classes target incretin pathways but differ in administration routes, with DPP-IV inhibitors available orally and GLP-1 agonists typically administered via injection.
Mechanisms of Action: How DPP-IV Inhibitors and GLP-1 Agonists Work
DPP-IV inhibitors enhance endogenous incretin levels by preventing the enzyme dipeptidyl peptidase-4 from degrading GLP-1 and GIP, thus prolonging their glucose-dependent insulinotropic effects. GLP-1 agonists mimic native GLP-1 by directly binding to GLP-1 receptors, stimulating insulin secretion, suppressing glucagon release, and slowing gastric emptying. Both mechanisms improve glycemic control, but GLP-1 agonists provide more potent receptor activation and additional benefits like weight loss.
Efficacy in Glycemic Control: A Comparative Overview
DPP-IV inhibitors and GLP-1 agonists both target incretin pathways but differ significantly in glycemic control efficacy. GLP-1 agonists generally provide superior reductions in HbA1c levels, often lowering A1C by 1.0-1.5%, compared to DPP-IV inhibitors which typically reduce A1C by 0.5-0.8%. Your choice between these medications can be informed by the need for more robust glycemic control associated with GLP-1 agonists versus the oral convenience and favorable safety profile of DPP-IV inhibitors.
Impact on Weight: Benefits and Differences
DPP-IV inhibitors primarily stabilize endogenous GLP-1 levels, resulting in a neutral effect on weight, while GLP-1 agonists provide a more potent and sustained activation of GLP-1 receptors, often leading to significant weight reduction. Clinical studies reveal that GLP-1 agonists, such as liraglutide and semaglutide, can induce weight loss ranging from 3% to 10% of body weight, whereas DPP-IV inhibitors like sitagliptin generally do not promote weight loss. The weight benefits of GLP-1 agonists are attributed to delayed gastric emptying and increased satiety, contrasting with the weight-neutral profile of DPP-IV inhibitors.
Cardiovascular Outcomes: Risk and Protection
DPP-IV inhibitors show a neutral effect on cardiovascular outcomes with no significant increased risk or pronounced protective benefits, as demonstrated in major trials like SAVOR-TIMI 53 and EXAMINE. GLP-1 agonists, such as liraglutide and semaglutide, consistently reduce major adverse cardiovascular events (MACE) including myocardial infarction, stroke, and cardiovascular death in patients with type 2 diabetes at high cardiovascular risk. Clinical guidelines favor GLP-1 receptor agonists for cardiovascular protection due to their proven efficacy in reducing heart failure hospitalizations and improving overall cardiovascular survival.
Safety Profiles and Common Side Effects
DPP-IV inhibitors generally exhibit a favorable safety profile with common side effects including mild upper respiratory infections, headaches, and nasopharyngitis, while serious adverse effects remain rare. GLP-1 agonists often cause gastrointestinal symptoms such as nausea, vomiting, and diarrhea, especially during treatment initiation, and carry a potential risk of pancreatitis and thyroid C-cell tumors. Both drug classes require careful monitoring in patients with a history of pancreatitis, but GLP-1 agonists demonstrate greater weight loss benefits despite a higher incidence of gastrointestinal side effects.
Administration: Oral vs Injectable Therapies
DPP-IV inhibitors are administered orally, offering convenience and improved patient adherence compared to GLP-1 agonists, which require subcutaneous injections. The oral route of DPP-IV inhibitors like sitagliptin and saxagliptin provides ease of use, especially for patients with injection apprehension. In contrast, GLP-1 agonists such as liraglutide and exenatide necessitate injectable delivery, which can pose challenges but also ensures controlled release and potent glucose-lowering effects.
Patient Suitability and Selection Criteria
DPP-IV inhibitors are often preferred for patients with mild to moderate type 2 diabetes who require moderate glycemic control and have a lower risk of hypoglycemia, especially those with renal impairment due to their safety profile. GLP-1 agonists are suitable for patients needing significant weight loss and enhanced glycemic control, particularly those with obesity and cardiovascular risk factors, owing to their ability to promote satiety and improve cardiovascular outcomes. Selection criteria emphasize patient comorbidities, risk of hypoglycemia, weight management goals, and renal function to tailor the therapeutic approach effectively.
Cost and Accessibility Considerations
DPP-IV inhibitors generally offer a lower-cost option and are available in generic formulations, making them more accessible for patients with budget constraints or limited insurance coverage. GLP-1 agonists, while often more effective for weight loss and glycemic control, tend to be more expensive and may require injectable administration, which can limit accessibility in some healthcare settings. Insurance coverage and patient assistance programs play crucial roles in determining the affordability and availability of both drug classes.
Future Directions in Incretin-Based Diabetes Therapies
Future directions in incretin-based diabetes therapies emphasize enhancing the efficacy and durability of GLP-1 agonists while minimizing side effects compared to DPP-IV inhibitors. Advances include developing dual and triple agonists targeting multiple incretin receptors to improve glycemic control and promote weight loss. Your treatment options may increasingly benefit from personalized medicine approaches integrating novel incretin modulators with improved pharmacokinetics and patient adherence.
DPP-IV inhibitors vs GLP-1 agonists Infographic